Shoulder pain during the COVID-19 pandemic – is the increase in frozen shoulder cases real or apparent?
- 28 February 2021
- Posted by: invicta_ortho
- Category: Shoulder

One surprising aspect of the COVID-19 pandemic has been a notable increase in the frequency of patients presenting with symptoms of a frozen shoulder. The reasons for this are unclear, but are likely multi-factorial and I will give my two pence worth below.
The condition of frozen shoulder was first described in the early 20th century and is typically characterised by 3 distinct phases: “freezing” (pain), “frozen” (stiffness) followed by gradual “thawing”; the overall process on average lasting between 2-3 years. The majority of cases will resolve on their own without the need for any treatment at all, however a significant (up to 40%) of people will have ongoing symptoms. Most cases of frozen shoulder arise spontaneously in middle aged people (40-60 yrs) with no underlying cause, although there is quite often a history of minor injury. People with underlying medical conditions such as diabetes and thyroid problems (either under or overactive) are more susceptible, as are patients who have suffered a significant injury to their shoulder or have undergone surgery to the shoulder, breast or armpit.
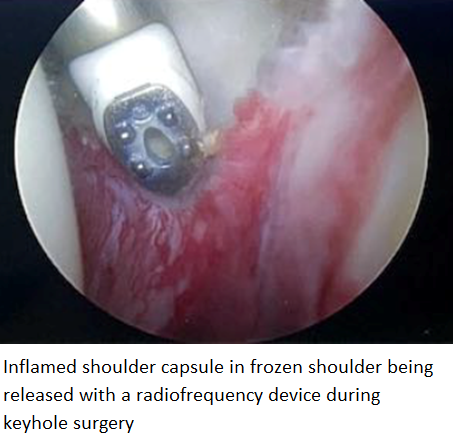 With a typical frozen shoulder there is no structural damage within the shoulder; by structural damage I mean significant injury to internal structures such as tendons, cartilage, nerves or ligaments. Patients often find this hard to believe given the severe pain they experience with this condition; often they describe feelings similar to a nerve being trapped or caught in some way as the intensity of pain can be eye-watering. The reason for this intensity of pain is that the lining of the shoulder joint (shoulder capsule) is often incredibly inflamed and swollen (see picture), particularly in the early phase of the condition. Inflammation and swelling anywhere in the body causes pain but as there is no external evidence of this with a frozen shoulder (the shoulder doesn’t get red or hot like in an infection), it can be difficult to conceptualise. Steroids are potent anti-inflammatory drugs, which is why they can be so effective at relieving the pain of a frozen shoulder, particularly in the early freezing phase.
With a typical frozen shoulder there is no structural damage within the shoulder; by structural damage I mean significant injury to internal structures such as tendons, cartilage, nerves or ligaments. Patients often find this hard to believe given the severe pain they experience with this condition; often they describe feelings similar to a nerve being trapped or caught in some way as the intensity of pain can be eye-watering. The reason for this intensity of pain is that the lining of the shoulder joint (shoulder capsule) is often incredibly inflamed and swollen (see picture), particularly in the early phase of the condition. Inflammation and swelling anywhere in the body causes pain but as there is no external evidence of this with a frozen shoulder (the shoulder doesn’t get red or hot like in an infection), it can be difficult to conceptualise. Steroids are potent anti-inflammatory drugs, which is why they can be so effective at relieving the pain of a frozen shoulder, particularly in the early freezing phase.
So why am I seeing more patients with frozen shoulder? Perhaps this is merely perception rather than reality – those patients with frozen shoulder, as they are relatively younger with more severe pain than the average patient with shoulder pain, may be more likely to want to take the small “risk” of attending a hospital to seek treatment at this time of the COVID-19 pandemic. Therefore, out of the reduced number of patients attending hospital during the pandemic, those with frozen shoulder might represent a greater proportion. Alternatively, there could be a direct causal effect, perhaps due to the increased frequency of home working and being hunched over a computer with poor posture. A lack of core strength and poor posture is known to lead to joint pain. Perhaps there is also a linkage to the increased emotional stress that people have been under during the pandemic. It is most likely, in my opinion, to be a combination of these factors.
I would encourage any patient who thinks they may have a frozen shoulder to seek specialist advice for a clinical assessment. Not only will you get the correct diagnosis, but the treatment options to enable you to get back to a more normal life are generally simple, low risk and effective.
David Rose

Consultant Orthopaedic Shoulder Surgeon MBBS FRCS (Tr.& Orth.)